ID Pain: A Neuropathic Pain Screen
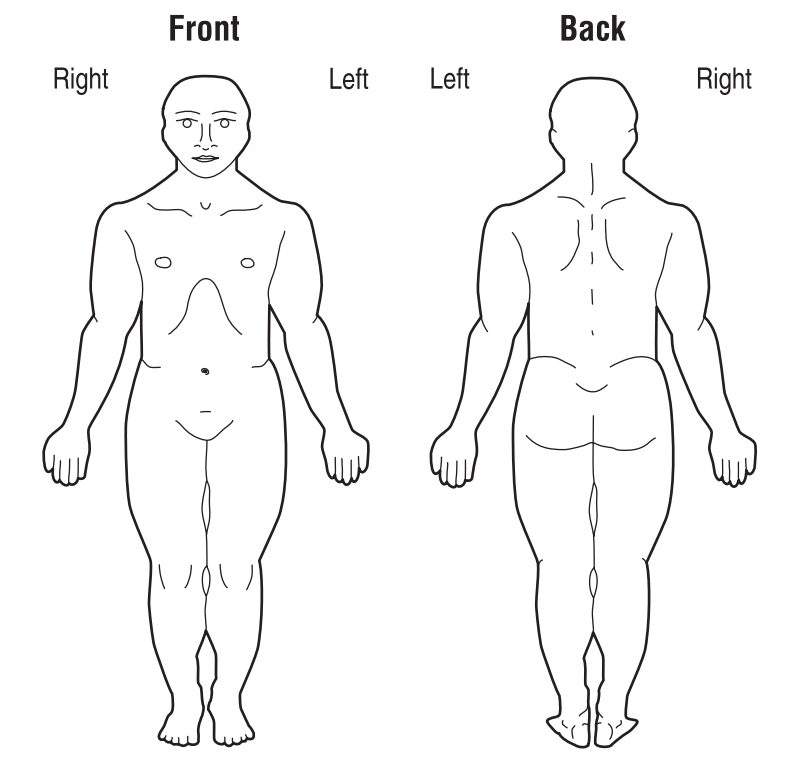
On the diagram below, shade in the areas where you feel pain. If you have more than one painful area, circle the area that bothers you the most.
Mark ‘Yes’ to the following items that describe your pain over the past week and ‘No ’to the ones that do not.
| Questions | Score | |
|---|---|---|
| Yes | No | |
| 1. Did the pain feel like pins and needles? | 1 | 0 |
| 2. Did the pain feel hot/burning? | 1 | 0 |
| 3. Did the pain feel numb? | 1 | 0 |
| 4. Did the pain feel like electrical shocks? | 1 | 0 |
| 5. Is the pain made worse with the touch of clothing or bed sheets? | 1 | 0 |
| 6. Is the pain limited to your joints? | -1 | 0 |
Portenoy, R. (2006). Development and testing of a neuropathic pain screening questionnaire: ID Pain. Current Medical Research and Opinion, 22(8), 1555–1565.